



Measles Vaccine, a real moneymaker out of nothing.
In 1962, a year marked by remarkable global changes and cultural transformations, astronaut John Glenn made history on February 20 by becoming the first American to orbit Earth in the Mercury spacecraft Friendship 7. This achievement represented a significant victory in the Space Race and highlighted the intense technological competition of the Cold War. Later that year, the Cuban Missile Crisis emerged—a fraught 13-day confrontation between the United States and the Soviet Union that nearly escalated into nuclear conflict, revealing the precarious nature of peace during the nuclear era. August brought shock and sorrow to the world with the unexpected death of Marilyn Monroe, the celebrated actress whose passing at just 36 years old led to widespread grief and ongoing debate about the circumstances of her suspected overdose.
The following year, 1963, would bring a highly anticipated medical breakthrough with the approval of the first widely administered measles vaccine in the United States. During 1962, measles was a frequent childhood disease, typically resolving on its own, though it sometimes caused serious complications and, in rare cases, death.
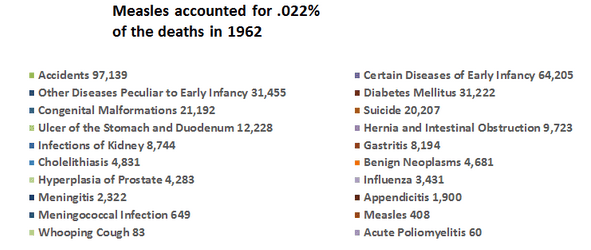
The chart above illustrates the primary causes of death in 1962. However, a more detailed examination reveals that these categories lack context and fail to capture the complexities involved. They focus on immediate causes but omit the wider social, economic, and systemic factors that influence mortality rates.
Measles, responsible for 408 deaths in 1962 and ranking 36th (accounting for only 0.022% of total deaths), occurred before the introduction of its vaccine, representing a minor portion of the chart. Of those 408 cases, serious malnutrition was involved in 70% of them.
In contrast, syphilis (ranked 30th with 2,811 deaths, or 0.15% of total mortality) and scarlet fever (ranked 38th, causing 102 deaths, about 0.006% of all deaths) are acute infectious diseases that seldom receive public attention, possibly because no vaccines are available for these illnesses.
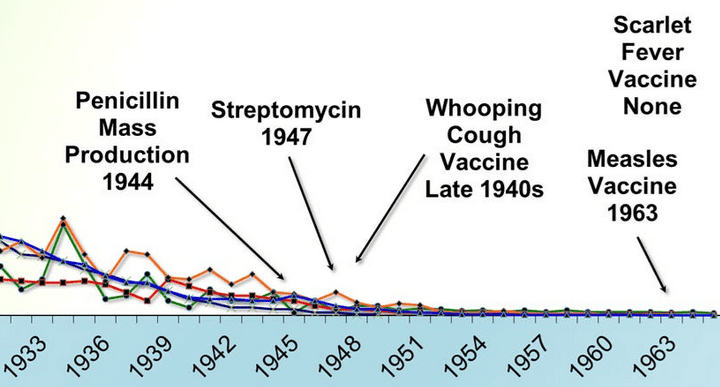
Despite vaccination efforts, whooping cough, diphtheria (for which the DTP vaccine was introduced in the late 1940s), and polio (with vaccines available since 1955) still claimed lives.
Tuberculosis is particularly significant, ranking 17th with 9,506 deaths (approximately 0.52% of total mortality). Although the BCG vaccine existed and was employed in various countries, it was never incorporated into routine immunization programs in the United States, partly due to doubts about its inconsistent effectiveness and a perception of low domestic risk.
Focusing specifically on the New England region—characterized by relatively high living standards and better healthcare access—measles mortality in 1962 was notably low, with just five deaths reported across all six states.
Connecticut reported zero deaths.
Maine had one death.
Massachusetts recorded no deaths.
New Hampshire reported zero deaths.
Rhode Island had one death.
Vermont accounted for three deaths.
When compared to the current urgent warnings about measles, these numbers are remarkable. The data from 1962 indicate that by the early 1960s—before the vaccine was introduced—measles mortality had already decreased considerably across many areas of the United States, particularly in wealthier regions such as New England. Enhancements in nutrition, sanitation, medical care, and living standards were crucial factors in lowering the death rate well before vaccines came into use.
Furthermore, these figures omit several vital factors contributing to mortality, such as medical mistakes, poor nutrition, poverty, environmental hazards, and systemic inequalities. By overlooking these fundamental health determinants, the pie chart reduces intricate causes of death into simplistic categories, prompting a crucial question: do these classifications accurately reflect the underlying reasons for mortality, or do they merely represent its ultimate manifestations?
It is important to highlight that public health reports often concentrate on the availability or absence of vaccines, rather than considering the broader context influencing health outcomes. This focus on isolated interventions can conceal the importance of comprehensive public health strategies that encompass access to healthy food, clean water, adequate housing, education, and quality medical care.
Examining mortality data from 1962 reveals that numbers alone cannot convey the entire narrative. Although the measles vaccine was introduced a year later in 1963, the previous year’s data illustrate a far more intricate scenario—with measles causing only a small proportion of deaths even before widespread immunization. This compels us to question the oversimplified stories commonly accepted and to delve deeper into the social conditions affecting health outcomes. Failing to consider the broader social, economic, and environmental influences on mortality risks distorting the true nature of the challenges we face and missing out on the most effective and lasting solutions.
1. Cardiovascular and Renal Diseases of Major Importance — 968,809 fatalities (53.20%)
2. Malignant Tumors — 278,562 fatalities (15.30%)
3. Accidental Deaths — 97,139 fatalities (5.33%)
4. Certain Early Infancy Diseases — 64,205 fatalities (3.53%)
5. Pneumonia — 56,564 fatalities (3.11%)
6. Other Various Diseases — 52,173 fatalities (2.87%)
7. Diseases Specific to Early Infancy — 31,455 fatalities (1.73%)
8. Diabetes Mellitus — 31,222 fatalities (1.71%)
9. Injuries During Birth — 28,199 fatalities (1.55%)
10. Liver Cirrhosis — 21,824 fatalities (1.20%)
11. Congenital Defects — 21,192 fatalities (1.16%)
12. Suicide — 20,207 fatalities (1.11%)
13. Other Pulmonary Diseases of the Bronchial Region — 20,072 fatalities (1.10%)
14. Symptoms Associated with Senility and Vague Conditions — 19,730 fatalities (1.08%)
15. Stomach and Duodenal Ulcer — 12,228 fatalities (0.67%)
16. Hernias and Intestinal Blockages — 9,723 fatalities (0.53%)
17. Tuberculosis — 9,506 fatalities (0.52%)
18. Homicides — 9,013 fatalities (0.49%)
19. Kidney Infections — 8,744 fatalities (0.48%)
20. Gastritis — 8,194 fatalities (0.45%)
21. Various Other Infectious Diseases — 5,791 fatalities (0.32%)
22. Asthma — 4,896 fatalities (0.27%)
23. Gallstone Disease (Cholelithiasis) — 4,831 fatalities (0.27%)
24. Benign Tumors — 4,681 fatalities (0.26%)
5. Bronchitis — 4,665 fatalities (0.26%)
26. Neonatal Infections — 4,551 fatalities (0.25%)
27. Prostate Hyperplasia — 4,283 fatalities (0.24%)
28. Influenza — 3,431 fatalities (0.19%)
29. Anemia — 3,398 fatalities (0.19%)
30. Syphilis — 2,811 fatalities (0.15%)
31. Meningitis — 2,322 fatalities (0.13%)
32. Appendicitis — 1,900 fatalities (0.10%)
33. Acute Nephritis — 1,572 fatalities (0.09%)
34. Complications During Delivery and Pregnancy — 1,465 fatalities (0.08%)
35. Meningococcal Disease — 649 fatalities (0.036%)
36. Measles — 408 fatalities (0.022%)
37. Dysentery — 323 fatalities (0.018%)
38. Scarlet Fever — 102 fatalities (0.006%)
39. Whooping Cough — 83 fatalities (0.005%)
40. Acute Poliomyelitis — 60 fatalities (0.003%)
41. Diphtheria — 41 fatalities (0.002%)
The Greatest Ever Deception on Mankind
The Smallpox Vaccine
Not only did it not work, it made the infections worse.
The medical profession holds a most false relationship to society. Its honours and financial rewards are measured, not by the good, but by the evil it does. The physician who keeps some member of the family of his rich neighbour on a bed of sickness for months or years, may secure to himself thereby both fame and fortune; while the one who would restore the patient to health in a week or two, will be neither appreciated nor understood.
Russell Thacher Trall, MD, 1872
This is a workingmans version of an article by Roman Bystrainsk.
You can find the full article with all the notations on romanbystrainsk@substack.com
For decades, vaccination has been deeply ingrained in the medical community, legal system, and society at large. However, as a new generation of doctors began their careers and started administering vaccines, they encountered a disturbing reality. Despite their initial enthusiasm for vaccination, rooted in their education and societal upbringing, they soon discovered a disconnect between the promised benefits and the actual outcomes. The notion that vaccination was a safe and life-saving practice, perpetuated by Edward Jenner's claims, began to unravel.
A notable example is Dr. William Jefferson Guernsey, a young physician from Philadelphia, who took over his father's smallpox cases in 1875. Like his peers, he vaccinated patients of all backgrounds, driven by his conviction and adherence to the prevailing medical norms. However, as he treated more patients, he began to notice discrepancies between the expected results and the actual outcomes. The more he witnessed the failures and adverse reactions, the more he questioned the dominant narrative. It took a significant number of cases with severe reactions, cowpox infections, and vaccination failures to prompt him to reevaluate his stance.
Dr. Guernsey eventually realized that it was more lucrative and convenient to comply with the Health Boards' requirements, rather than risking his reputation and income by speaking out against the practice. He was horrified by the legal obligation to perform a medical procedure that he deemed questionable and even more disturbing, the fact that patients were forced to undergo vaccination in order to attend schools they were taxed to support.
Many other medical professionals found themselves trapped in a similar predicament, facing the threat of legal repercussions, financial losses, and professional ostracism if they dared to challenge the vaccination status quo. Here is a rewritten version of the text:
Despite their reservations, the majority of individuals felt compelled to vaccinate due to the triple threat of pressures. However, a select few doctors, driven by their unwavering integrity and perseverance, dared to defy the prevailing medical opinion and challenge the vaccination procedure.
One such doctor was Robert A. Gunn, MD, who graduated in 1866 and initially subscribed to the notion of vaccination. Between 1870 and 1872, a global smallpox epidemic swept across the world, including New York City, which had been deemed thoroughly protected by vaccination. As part of an investigative committee, Dr. Gunn uncovered disturbing evidence: despite a 95% vaccination rate, the number of smallpox cases and mortality rates had reached unprecedented levels, surpassing those of the entire century.
This revelation prompted Dr. Gunn to embark on an exhaustive study of the subject. He delved into the works of Jenner, the supposed pioneer of vaccination, as well as reports from the Registrar General of England and various health boards across the United States. His investigation revealed a startling pattern: nearly every smallpox patient had been vaccinated, with many having received the vaccine recently.
Dr. Gunn's critique of vaccination earned him a reputation, and subsequently, hundreds of children were brought to him each year, suffering from a range of debilitating conditions, including swollen arms, ulcers, erysipelas, and skin eruptions. In countless cases, these children's health was irreparably damaged for life.
Over three decades, he dedicated himself to an in-depth examination of the vaccination debate. His research revealed that most physicians unquestioningly accepted the safety and efficacy of vaccination, without conducting their own investigations. After years of meticulous study, he reached a stark conclusion:
The practice of vaccination, in my opinion, is the most misguided and harmful of all dogmas. I firmly believe that not a single individual has ever been shielded from smallpox through vaccination, while numerous cases of severe bodily harm and even fatalities have resulted from its use. The entire theory is based on unfounded assumptions that defy common sense and contradict established principles of physiology. Experienced physicians have encountered countless instances of skin eruptions, erysipelas, and syphilis that can be directly attributed to vaccination. If these cases were compiled into a single report, they would paint a more alarming picture than even the most horrific accounts of smallpox.
Similarly, Dr. Montague R. Leverson, a staunch advocate of vaccination, had been taught from a young age and throughout his medical education that vaccination was a harmless and effective safeguard against smallpox. However, a case he encountered in January 1894 prompted him to conduct an exhaustive study on vaccination. For eight years, he devoted an average of four hours a day, and sometimes up to 16 hours, to investigating the pathology of vaccination and smallpox. Ultimately, he was forced to conclude that:
The medical profession has been plagued by numerous fads, but none as abhorrent as the practice of injecting healthy individuals with the putrid matter of an animal disease. I must emphasize to the members of the Medico-Legal Society that there is no credible evidence to suggest that vaccination has ever prevented or will prevent an outbreak of smallpox, except in cases where the patient succumbs to the vaccine itself before contracting the disease.
For nearly two centuries, our profession has burdened humanity with a pernicious superstition and oppressive tyranny. Through inoculation and vaccination, we have contaminated the blood of humanity, catering to the power-hungry ambitions of the ignorant, greedy, and conscienceless. Despite the contributions of a few genuine physicians, our profession has been a blight on humanity throughout its existence.
Dr. Charles Creighton, a renowned professor at the University of Cambridge, is celebrated as a pioneer in British epidemiology. As one of the most erudite medical scholars of 19th-century Britain, he exerted a profound influence on the intellectual landscape of his time. His meticulous research and numerous writings earned him a reputation as a leading authority. His magnum opus, "History of Epidemics in Britain," is hailed as a paragon of accuracy.
In 1884, Dr. Creighton was commissioned to write an article on vaccination for the 9th edition of the Encyclopædia Britannica. Instead of regurgitating conventional wisdom, he embarked on an exhaustive examination of pro- and anti-vaccination literature from around the world. Initially, he shared the prevailing views on vaccination, but his rigorous investigation eventually led him to challenge the dominant opinions held by his peers.
When I commenced my research into vaccination in 1886, I was not immune to the prevailing biases that favoured established doctrine and practice. However, after months of meticulous research, I felt compelled to revise my opinions, which I had previously accepted without question.
In 1888, Dr. Creighton's groundbreaking research on vaccination was featured in the Encyclopaedia Britannica. Around the same time, he published two seminal works: The Natural History of Cow-pox and Vaginal Syphilis, and Jenner and Vaccination: A Strange Chapter of Medical History. These meticulously researched publications presented compelling evidence that challenged the dominant views on vaccination, ultimately leading Dr. Creighton to conclude that the practice was based on a "grotesque superstition." His provocative findings sparked controversy within the medical community, exposing the deep-seated nature of beliefs that had been passed down through generations. Dr. Creighton came to realize that the influence of ancestral traditions continued to shape the decisions of modern-day individuals, who relied heavily on the assurances of their predecessors.
As long as the medical profession continues to uphold the Jennerian doctrine of vaccination, it remains tied to the outdated thinking of the eighteenth century. The history of vaccination, from its inception to its current state, serves as a stark reminder that medical science is often driven by human biases rather than scientific objectivity. The refusal of medical leaders to acknowledge and correct their mistakes has become an inherited obligation, with each successive generation feeling bound to uphold the flawed theories of their predecessors. Today, anyone who attempts to defend Jenner's theories must be prepared to sacrifice their reputation for scientific and historical accuracy. Consequently, many individuals with a reputation to protect decline to take on this challenge.
The widespread trust in vaccination persists largely because people struggle to accept that a respected profession, driven by scientific principles, could have been mistaken for such a long time. It's difficult for the general public to comprehend how a prestigious profession could have been so consistently wrong. As Carlyle's maxim states, "An error is not fully refuted until we understand not only that it's an error, but also how it came to be." When I began this book, I sought to understand how the medical profession worldwide fell under the illusion of vaccination. I believe they were primarily misled by the term "cowpox," which was used to introduce the new protective measure. Jenner bears sole responsibility for this initial error, which was flawed from its inception and further compromised by its secretive publication. The medical profession has historically upheld erroneous doctrines and harmful practices, which were supported by its authority for generations.
Dr. Creighton's newfound awareness led him to realize that questioning vaccination would come at a significant personal cost. Despite his exceptional credentials, intellect, and meticulous research, his comments hinted that both he and his groundbreaking work would ultimately be dismissed and relegated to the margins of medical history.